As I see it
Philip James

Access Philip James's profile here
Riyadh, Saudi Arabia. Everybody who is familiar with the Middle East will recognise the astonishing transformation in the region's health over the last 40 years. When I was establishing a new public health nutrition teaching programme at the London School of Hygiene and Tropical Medicine in the early 1970s, childhood malnutrition as well as zinc and iron deficiencies with high infant mortality rates dominated the Middle East. At that stage life expectancy was low. Later, when I was director of the Rowett Research Institute, at a Founder's Day, a retired General from the British Army described in graphic detail the time when he was in charge of trying to feed not only 6-7 million semi-starving displaced people in Europe immediately after the 1939-1945 war, but also having to cope with a similar number in the Middle East. This was the time when the British were making such a mess of coping with the dual interests of the Palestinians with those of the Jews who were intent on creating an Israeli state.
Since then I have been all too conscious of the transformation in the health profile of the region, having spent many years visiting my own family in Abu Dhabi, and also lecturing throughout the region. By virtue of running the International Obesity Task Force (IOTF) with all its interactions with WHO, I often found myself talking to national government ministers of health, but I could never persuade them to focus on issues of cardiovascular and diabetes prevention. All they could think about were better treatment and drugs such as the potential wonders of a 'poly pill'.
Now things are being transformed. Ala Alwan, who was in charge of the World Health Organization non-communicable diseases programme in Geneva, has now taken up his position as regional director of the WHO Eastern Mediterranean Regional Office (EMRO). This interacts with 22 countries with a somewhat curious distribution. The North African countries of Algeria, Tunisia and Morocco as well as Egypt and the Sudan are included. Turkey is excluded, but Pakistan is brought in I guess to keep it apart from India. Israel, of course, is assigned to the European Region for similar political reasons.
When I was visiting WHO in Geneva earlier this year with Association president Barrie Margetts, Ala Alwan made it clear that he regarded the EMRO region as in real need of dramatic developments in public health. As soon as he took up his post last February, he began to plan a new initiative. This came to fruition in Riyadh last month, between 9-12 September, where 21 of the 22 Ministries of Health were involved, with Saudi Arabia taking the lead and providing a huge amount of support for the regional conference.
Transformation of life and disease
The opening ceremony was replete with members of the royal families, national ministers and very senior officials. Ala Alwan highlighted the dramatic changes that have occurred over the last 40 years. He described the 20 year increase in life expectancy and the plummeting infant mortality rates since the 1970s, with a non-communicable disease epidemic that had emerged more rapidly than in any other part of the world. Already in some countries, the four diseases that were highlighted in the UN General Assembly high-level meeting last September – cardiovascular diseases, cancers, chronic respiratory diseases and diabetes – now account for more than 80 per cent of deaths. Indeed, six of the ten countries with the highest prevalence of diabetes in the world are located in this Eastern Mediterranean region.
Despite the evident luxury in Riyadh and our conference environment, we were soon reminded of the huge problems confronting the region, with poverty and huge political unrest as well as civil war in Syria. The challenge for the conference was: what can be done to cope in a region with such huge political challenges?
We were vividly reminded by Chris Murray, with his many years of experience at WHO Geneva, that the region was now confronting a massive economic and social problem. With his usual brilliant mathematical and presentational skills, he showed moving pictures of the changing patterns of disease. It became apparent that even as recently as 1990, nutritional deficiencies were still a major regional feature. Now, however, non-communicable diseases have reached catastrophic proportions.
He was followed by Majid Ezzati, who also has been spending the last three or so years recalculating the global burdens of disease and their principal risk factors. These data were originally going to come out last March, but now we learned on the grapevine that they will feature in a single big issue of The Lancet soon, probably in early December. We had just a glimpse of the issues but it was already apparent that weight gain and obesity were the single most important risk factors determining the health burden of the Gulf States and I think of the whole region. It would appear that when we finally see the new analyses, nutritional issues underlying non-communicable diseases will become much more prominent.
Whereas the UN General Assembly high level meeting highlighted only the problems of salt reduction and trans fat elimination as important, the view of the New York meeting was that other issues were to be dealt with merely by 'increasing public awareness about diet and physical activity'!
Table 1
Multi-sectoral engagement
to reduce non-communicable disease risk factors
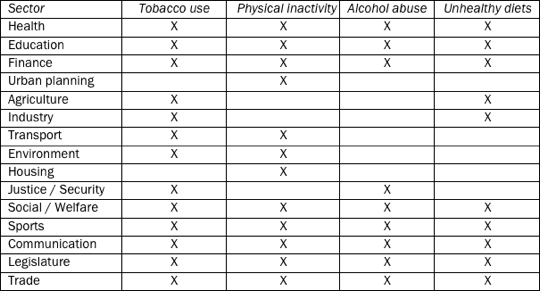
In the Riyadh conference the failure of many countries to implement the full range of measures in the Tobacco Framework was highlighted. Interestingly, alcohol was also a surprisingly big problem. In the background documents that the WHO EMRO regional office had circulated, the fundamental role of multisectoral engagement was highlighted, with lists of all the departments of government that should be involved in dealing with tobacco use, physical inactivity, alcohol abuse and an unhealthy diet. See Table 1, above. I would go a little further. At the conference I noted that unhealthy dietary patterns also have environmental determinants, and many will insist that urban planning, transport and housing should also be considered as influencing dietary patterns, given the current intense interest in urban agriculture and the need to increase local food production and minimise carbon emissions.
The Riyadh Declaration
The conference had the usual separate meetings on the major individual risk factors. Some of the most intriguing responses came when the preliminary draft of the Riyadh Declaration was produced overnight. I had set out, in an early presentation, the fundamental need to reconsider the whole food system and how best to cope with the influence of the Western diet in a 'free market' system which is guaranteed, in any society where malnutrition has recently been prevalent, to produce even greater burdens than those now afflicting the US or Western Europe.
This theme of changing the food system came through powerfully, but curiously the Saudi Minister of Agriculture, in his speech, seemed exclusively focused on the need to develop organic farming in Saudi Arabia. I don't think that anybody had really considered the wide range of issues involved in shifting the agricultural emphasis, but they did understand the major dilemma of how best to increase physical activity in countries where, in summer the temperature may rise to 45 or more degrees Centigrade.
Salt reduction
At the conference, Graham MacGregor of World Action on Salt and Health did his usual excellent job of driving home the need for salt reduction and illustrated it with his numerous examples of what was needed from his UK experience. Ala Alwan agreed with several national ministry representatives present that this was an immediate priority, so there will be a special WHO EMRO consultation on salt reduction at the end of November in their main office in Cairo. Representatives from Oman worried about the need to safeguard the iodisation of salt given the very substantial problems of iodine deficiency in the region.
I was also classified by my good friend Graham as a rather critical pessimist because I saw the salt reduction programmes as much more complicated in societies where processed food is probably not nearly such a dominant feature as in North America or Western Europe. Up to 80 per cent of salt in some lower income countries comes from home use. However, my guess is that in the Middle East region and many middle income countries, we have three major sources to consider. The first is salt use in the home, but the second and perhaps very important input comes from street foods and other fast food outlets, rather than from processed foods which is the main source in countries like the US and UK. In many of the Middle East countries, with huge migrant servant populations, much of the cooking at home is actually done by employees from abroad which is yet another challenge.
Profiling and labelling
Another issue I am grappling with is nutrient profiling and traffic light labelling, which we first developed when I was responsible for the UK Coronary Prevention Group in 1986. This was immediately recognised by most Riyadh conference participants as important, but it became clear that the biggest problem for ministries of health is to convince other branches of government that anything needs to be done. These other ministries are dominated by their own economic priorities and see these health issues as almost irrelevant for them. We talked to several officials who told us how frustrated their ministers of health were with the failure of their attempts to persuade their ministerial colleagues and policy groups to take account of health issues in their various departments.
Francesco Branca from WHO in Geneva, speaking at Riyadh, was determined to ensure that the range of nutritional issues should be properly considered. He certainly made some impact because the final Riyadh Declaration, (please use the link here) which the Minister of Health set out at the end of the conference in Arabic, followed by my own presentation of the English version, included much more than a vague reference to increasing public awareness of dietary issues.
It was agreed with Ala Alwan that once we have dealt with salt, then we need to get into the whole issue of other dietary questions and link trans fats with the need to reduce saturated fat and I believe also total fat, with an adjustment in the omega 6/ omega 3 ratios. The high consumption of fruit juices and sweetened soft drinks in the Middle East has also been neglected. Given the major emphasis on banning alcohol in several countries, it was no surprise to me that I was bombarded with offers of huge glasses of any one of 20 different types of fruit juice, with or without added sugar.
How can a change in public health policy be accelerated, given that countries undergoing explosive nutrition transition need to take a really radical approach? The 'whole lifecourse' approach seemed to be generally accepted, but we still do not have the vivid illustrations of how so many previously malnourished babes and children are now already succumbing to the problems of glucose intolerance and all the other risk factors which already affect a huge proportion of the Middle East populations. Let us hope that Ala Alwan, with all the help he can get from our community, can trigger a revolution in thinking and a new approach in a region which has really neglected public health nutrition as a major public priority for at least a quarter of a century.