2013 March Column
Philip James


The WHO Eastern Mediterranean region (at left). The 'Fertile Crescent',
the cradle of Egyptian, Greek, Roman and European civilisation (at right)
Cairo. This is where I have been, at a series of meetings convened by Ala Alwan, director of the WHO Eastern Mediterranean Regional Office. The region, as well as Lebanon, Syria, Palestine, Jordan, Libya and Egypt (Cairo being the headquarter rs), and the Arab states, includes Iran and Iraq, Tunisia, Morocco and both Sudans (see above, left), and Pakistan and Afghanistan. One of my tasks was to advise on possible progress after the ending of the 2000-2015 Millennium Development goals, in the new 2015-2025 period now being urgently planned.
The whole region needs waking up to what are now appalling increases in rates of obesity, and of diabetes and related diseases. Yet at the same time, there is plenty of 'classic' undernutrition and food insecurity, and high rates of infant and maternal mortality, caused by poverty, lack of basic services, poor education, unemployment, and urban chaotic squalor. All this is made worse by political and economic instability, violence, and various types of war caused by factors I will not go into here. All this besets a region that includes the Garden of Eden, and the Fertile Crescent, the cradle of Egyptian, Greek, Roman and thus European civilisation (see above, right). It has been a chastening experience.
Lancet series. Chronic non-communicable diseases
Towards 2015-2025

The Lancet has marshaled another impressive series, this time on how to shape and meet the 2015-2025 goals to prevent and control chronic diseases
Because of being away in Cairo, I missed the launch in London of the new Lancet series, also on the theme of shaping and meeting the planned 2015-2025 development goals. There's an account of the launch on the home page of this issue of the Association's website.
I have borrowed its line-up of pictures shown above, to make the point that the process of producing the series of Lancet series on any specific topic is impressive. As well as editor Richard Horton (left, above), the process also involves an overall guiding group, who this time included (next on the left) former New Zealand premier Helen Clark, her long- time friends former WHO executives Ruth Bonita and Robert Beaglehole, and former PAHO director George Alleyne. Such a group shapes the process that leads to topics for papers and lead authors being selected to work with specific co-authors (like the three on the right). The lead authors produce proposals and then there is often a meeting in London, where the authors meet, and referees are invited to advise, prior to the usual process of series of successive drafts moving towards submission, review, editing and publication. Then there is a launch of each series, at a prestigious location in London, with simultaneous publication on-line and in print.
The current series has obviously been very carefully coordinated and managed. One of the papers is on 'Profits and Pandemics', co-authored by the three people on the right above, Rob Moodie, David Stuckler, Carlos Monteiro, and others (1). Their paper does not take a medical approach, but highlights the remarkably similar strategies that many transnational tobacco, alcohol and food corporations use to drive into and thoroughly penetrate the markets of what we used to call the 'developing world'. The data, some taken from David Stuckler's papers in PLoS Medicine last year, show how we who are engaged with public health nutrition, need to focus on industrial and trade policies rather than remaining preoccupied with systematic reviews and microanalyses of clinical trials.
Prevention of chronic disease in the Middle East
Policies and realities
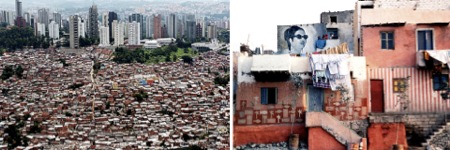
The realities of Cairo life. Self-built informal housing, with no security of tenure. The people who live here are not thinking about obesity or diabetes
Cairo was many worlds away from that of the gentle debates at The Lancet launches. When in Egypt I found that officials from the many countries I met were rarely aware of these Lancet series, including – apart from WHO officials involved in the topic – the new Global Burden of Disease series I reviewed in January (2,3). I should not have been so surprised. There were up to five daily street demonstrations in Cairo, as well as major political rallies very Friday and rioting in several cities in Egypt, while I was there. In addition the carnage in Syria continues, with UN officials anguished at all the suffering and the seeming inability of foreign governments to intervene.
I had several discussions with Ala Alwan while in Cairo. A substantial proportion of the countries in the region are involved in civil wars, terrorism, or political and economic turmoil. WHO officials and staff have the duty to remain accepted by both sides in any conflict so that with the Red Crescent and medical relief workers, they can help to meet the needs of the stranded communities even in the most war-torn parts of a country. Several UN and other workers trying to eradicate polio in Pakistan had just been killed by insurgents who considered polio immunisation to be some form of Western plot. A maternal and child summit in Dubai in late January had highlighted the shocking mortality rates of mothers and their children in several countries. A cancer team had just returned from Yemen where there is only one specialist cancer treatment centre in the whole country. This gives just a snapshot of what WHO has to contend with on a frequent if not daily basis.
On a previous visit to Cairo discussions were abruptly ended as a WHO team came in to report on emergency care and food plus medical supplies for Afghanistan, and resting for one night in Cairo, before leaving for Somalia the next morning on a similar mission. In such contexts plans to improve public health by improving national food systems and supplies, are likely to have a low priority.

The realities of Cairo. These riots here were triggered by insecure bread supplies. People fighting for basic food do not think about heart disease
On this visit I took part in a global diplomatic summit involving ambassadors and other senior officials and policy-makers from 18 WHO Eastern Mediterranean countries. The issue of priorities was paramount. Ala Alwan was supported by Ilona Kickbusch, whom I know well from her days working for the WHO European regional office in Copenhagen. She is one of the outstanding thinkers on how best to ensure that health is taken into account inthe diplomatic rounds that shape international and national policies on trade, economic development, sustainability, and the global financial crisis, all in the context of the current radical reorganisation of a resource-starved WHO (4).
This links with the one of the new Lancet papers, whose lead author was George Alleyne (5). How best can we ensure that the crisis of chronic non-communicable diseases becomes part of government and development agencies routine thinking? This in turn relates to planning for 2015-2025. For instance, last month there was a meeting in Monrovia, Liberia attended by David Cameron, the UK prime minister, who is one of the three chairs of a UN working party appointed by secretary-general Ban Ki-moon to shape the 2015-2025 agenda. On return to the UK Cameron said that the new plan will just focus on combating poverty. In Cairo I heard differently. Poverty as such is planned to be one of about five priorities within an integrated plan. Sustainability is a critical issue. So are climate change, water and environmental issues, and inequity, with a new version of 'health for all' as the overarching theme. The chronic non-communicable disease crisis problem may well be simply one item in a pot of multiple health issues.
Food systems
Can agriculture serve health?
My task at the Cairo diplomatic health summit was to address the agriculture and food systems that now are increasing the heavy burden of obesity and chronic non-communicable diseases that afflict the populations of Eastern Mediterranean countries. For the officials listening this was a novel concept. They readily accepted that the prevalence of obesity in women in much of the region is now the highest in the world (bar some Pacific islands), that up to 20 per cent of adults have type 2 diabetes (diagnosed or undetected) and that up to 30 per cent of adults are hypertensive (again, known or unknown).The diplomats and officials present will have known this, if only because they themselves, or family members and colleagues, were personally affected. But they clearly saw these as medical issues, to be addressed by government health departments spending more public and private money on hospitals and drugs (of a quality only affordable by insured or wealthy people) with maybe some education designed to promote 'healthy lifestyles'.
But when I went 'upstream', to consider the underlying and basic causes of obesity and the diseases that are now such appalling epidemics in their countries, they were I sensed, amazed or bemused. I pointed out that as everybody in the region knows, the food patterns of countries like theirs have been developed over very many centuries of agricultural production and food manufacture and distribution. These necessarily have been shaped by the extraordinary climate and terrain of the region, which in turn have shaped unique food cultures and their own versions of the Mediterranean diet, itself now so threatened that it is like the classic Mediterranean diet becoming a truly endangered feature of their culture.
It was not necessary to remind those present that outside China and Meso-America, the first systematic agriculture that transformed pastoralists into farmers started in and around the banks of the great Tigris and Euphrates rivers in what is now Iraq around ten millennia ago. This whole new way of securing food supplies spread throughout 'The Fertile Crescent' (see map above) that included and indeed created Egypt as an entity. It allowed the development of towns and then cities, including the first city of Jericho, and was the cradle of the Egyptian, then Greek and Roman, and then other European civilisations.
But now the food systems of the whole region are breaking down under the strain of rising populations, urbanisation, economic globalisation, and national factors better known to those present as part of their daily lives than to me. I tried to show how agriculture and food systems evolved over say 3,000 years are now being overwhelmed by changes taking place in the last 30 years or so. Notably, in tune with the new Lancet series (1,5,7), I stressed the vast power of the transnational agriculture, distribution and manufacturing corporations, whose impact is at least as great as that of the tobacco and alcohol transnationals. In common with these ruthless industries the agricultural/food industrial complex as it is sometimes known are already gaining their greatest profits by displacing the food systems and supplies of Asia, Africa, Latin America – and the Middle East.
There are also profoundly important issues in the region itself. I gave three examples: water, salt, and sugar.
Physical resources
The draining of water

The river Jordan in 1918 (right) and now (left). One of the great waterways
of the world has now in part become a ditch, drained for Israeli industry
I set out some fundamental issues, starting with water. Only 12 per cent of land in the North African and Eastern Mediterranean countries can be cultivated. A mere 5 per cent is fully fertile: 7 per cent of all the land is forested and 8 per cent is range land only able to support animals such as camels and oryx. The rest is desert.
The very rapid rise of urban and total populations has put an impossible strain on rural economies (8). Yet governments continue to allow building on this very scarce agricultural land with Cairo grabbing huge areas of precious growing fertile land with its now 20 million inhabitants. Israel has extracted so much water from the Jordan that this once mighty river in places now looks like a ditch (see above). The Nile is threatened, as I first knew when I studied malnutrition and its relationship with food insecurity in the Middle East at the London School of Hygiene in the early 1970s. What I did not realise then was the scarcity of land resources, with water supplies so limited that many countries for many years have either exhausted non-renewable water sources from deep reserves below the desert as in Libya. Or else, they are dependent on food imports to supply dietary energy and also what the Arab Water Council terms 'virtual water'. As shown in Figure 1, 'virtual water' is that used in other countries to grow the foodstuffs which the Arab and other nations in the Middle East import (9).Without this they would perish.
Figure 1
Virtual water in the Eastern Mediterranean
Water imported as contained within food grown in other countries
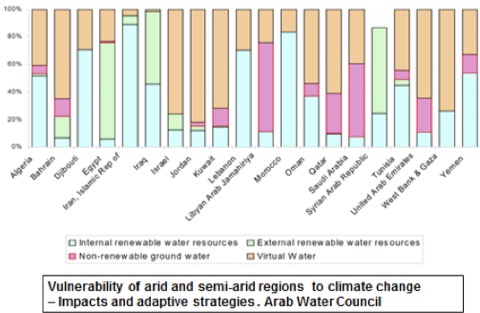
As you can see from the figure, Iran and Iraq are more or less self-sufficient in water, whereas countries in the arid Arabian region are desperately short. Many are dependent on external but renewable water. Thus the Nile flows from South Sudan through Sudan and only then enters Egypt. Similarly Syria and Iraq are dependent on other countries allowing an adequate flow of water into their country. This is a vivid example of the need for national, regional and potentially global diplomacy.
Hypertension. Salt
Salt is a big business

Extraction and production of salt goes back to the pre-agricultural era and shapes food cultures. Global salt production is now 200 million tonnes a year
Salt production predates agriculture, because in nature foods are short of sodium, an essential mineral, which is also a preservative used probably from the times when Palaeolithic people stored food from hunted animals (10). Total production of sea or rock salt is now around 200 million tonnes a year. Salt is big business.
The need to think in an industrial way and also to respect long-established food culture, was brought home to me vividly the day I arrived in Cairo. I joined a meeting of the Gates-funded organisation the Global Alliance for Improved Nutrition (GAIN), a large part of whose work is food fortification, together with a group of experts concerned with iodine deficiency. They were attempting to ensure that there were suitable levels of iodine in Egyptian salt. Urinary iodine analyses now indicate reasonable levels of iodine intake.
GAIN is one of the most powerful 'public-private partnerships', and the meeting was joined by executives from a dozen or so big salt producers. The salt business in the Middle East is huge. Most countries produce tens of thousands and even millions of tonnes of salt a year, most of which is exported for industrial use and I suppose for melting ice off the roads of the North in winter time. Special machinery is needed to add precise amounts of iodine to salt used for food. The Egyptian government is now no longer in a position to subsidise the process, being understandably more preoccupied with protecting the price of bread lack of which has been causing street fighting (see pictures above) but this seemed not to trouble the industry, whose executives were I imagine pleased that their product was helping to protect health.
So how much salt is consumed in Egypt? In the UK and other affluent countries, work to reduce salt consumption begins by examining food intake data and then assessing results by monitoring representative 24 hour urine collections. But in most Middle Eastern countries there are few reliable surveys or monitoring methods. There is certainly a problem of salt induced high blood pressure to contend with, as evident from the very high rates of hypertension: dietary studies in Turkey, Egypt and Jordan suggest that average intake may well be as high as 15 to 17 grams of salt per day. These levels would have seemed crazy and probably wrong to me before I witnessed in practice the intense saltiness of food offered to me in the restaurants and canteens during my 10 days stay.
Dietary surveys are valuable when they are done, but nutritionists in many countries often simply use US or UK food composition data to guess how much salt there is in roughly equivalent products in their shops and markets. The results then lead to hopeless underestimates of salt intake. It became obvious to me that the one reliable source of information is industry itself, whose managers will know to the tonne how much salt they provide to food companies, how much they sell to big catering groups, and the amount of salt that is sold as such.
Figure 2
Salt reduction: an industrial approach
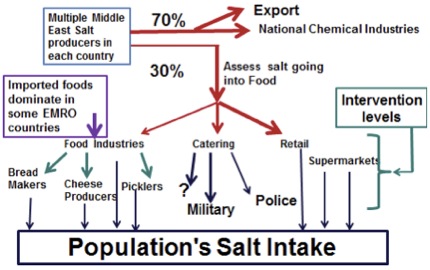
Figure 2 shows what emerged in Cairo. So what can be done to reduce salt consumption in the Eastern Mediterranean? Currently we have little idea of the proportion of salt being eaten from packaged and processed foods, from fast food and street food outlets, and from food eaten at home. We know that in high-income countries like the UK, Denmark and the Netherlands, about 85-90 per cent consumed comes from processed and packaged products. In Western Mediterranean countries until recently about half of salt consumed was added in the home in the preparation of meals. In relatively impoverished Latin American countries as much as 85 per cent is added in the home. So what about Eastern Mediterranean countries? The information will not come from surveys. The best answer may well come from work with industry itself.
So how given all this uncertainty can progress be made at a reasonable pace? Given the extraordinary history of conflict and government efforts to exert some control over a country's development, there are in many Eastern Mediterranean countries big publicly funded institutions, such as the army and police as well as government offices. They usually provide food as a routine on their premises so this means that their whole canteen systems could be improved. That would be a start. Big users of salt such as bread, cheese and pickle manufacturers can also be approached through their trade associations. Trickier issues such as food product imports, not to mention World Trade Organisation restrictions, could then be faced later.
This may sound a small effort. But Chinese studies show that when caterers supplying food to factory workers, soldiers and police reduce the salt in their food this, combined with advice to limit salt and also fat intakes at home, can lead to a 75 per cent fall in stroke rates within a 5-7 year period (11). These data do not comply with WHO's new demand for randomised intervention trials, but they are a brilliant demonstration of ways to transform population health. So we hope to engage the Egyptian army to lead both a coherent and politically important initiative, despite all the societal turmoil in the country. The army still seems to be respected, so if military health could be improved, this will be seen to justify parallel moves in other communities. A similar strategy may work in other countries.
Obesity. Sugar
Keeping Egypt sweet
Cane has been cultivated for sugar in Egypt perhaps since 1500 BCE (left)
and (right) Egyptians still enjoy extremely sweet drinks, cakes, desserts
I also talked with the diplomats about sugar. I had just discovered that sugar or something like it was refined in Egypt around 1500 BCE (above left). Sugar refining was certainly established as an artisanal industry by the 7th century AD. Sugar was a favourite of prosperous Egyptians over a thousand years ago, and ever since then the agriculture of the whole region has included sugar cane plantations and refining factories, and its food culture has incorporated intensely sweet coffee, cakes, sweets and desserts – and fruit and soft drinks, always on offer in the meetings I attended.
In the last 30 years production of sugar has trebled, and consumption has doubled, for Egyptians now are consuming sweetened Western-style products on top of their traditional sweetened foods and drinks. Industry figures indicate that average consumption is over 90 grams a day, which is close to 20 per cent of total food and drink energy intake, and this figure may well not include some of the sugar in imported products even if these values are meant o be included in the sugar available for consumption. These values I chose were from industrial sources which specify sugar consumption as a lot higher than UN Food and Agriculture Organization survey data indicate.
How can sugar consumption be reduced, in a country where production of sugar is important internal and external markets, where the traditional food culture includes intensely sweetened foods and drinks, and whose people are now exposed to branded sweet foods and drinks whose intensive marketing suggests that their consumption is part of the good life?
Will policy-makers pay attention to projections of rates of obesity and diabetes? I rather doubt it without some compelling political reason. They will need to do so at some point of course , and the sooner the better for the sake of their countries. The classic idea, much beloved by politicians and far too many nutritionists for my liking , of simply appealing to the public in public health education campaigns to reduce their consumption of sugar and salt, in the hope they will respond, seems very optimistic in the current intense turmoil in the Middle East,. Faced with insecure supplies of bread and fluctuating and rocketing prices, people will not be too fussy about the amount of salt in the bread they can obtain, and caffeine plus sugar "hits" from strong sweet coffee is of great solace for anxious and harassed citizens as well as those fighting for political change.
So after confronting reality in the Middle East and reinforced by reading The Lancet, I now regret that I have not paid far more attention to the industrial aspects of food systems.
References
- Moodie R, Stuckler D, Monteiro C, Sheron N, Neal B, Thamarangsi T, Lincoln P, Casswell S. Profits and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries'. The Lancet 2013.381:670-679. Published on-line on 12 February: http://dx.doi.org/10/ 1016/50140-6736(12)62089-3
- Lozano R, Naghavi W, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010, The Lancet 2012, 380, 9859, 2095-2128.
- Lim S, Vos T, Flaxman A, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in21 regions, 1990-2010: a systematic analysis for the Global Burden of DiseaseStudy 2010. The Lancet 2012; 380, 9859, 2224-2260.
- Kickbusch I, Rosskam B (eds). Negotiating and Navigating Global Health: Case Studies in Global Health Diplomacy. London: World Scientific, Imperial College, 2012
- Alleyne G, Binagwaho A, Haines A, Jahan S, Nugent R, Rojhani A, Stuckler D. Embedding non-communicable diseases in the post-2015 development agenda. The Lancet.2013, 381:566-574
- UK Government. Monrovia Communique. http://www.post2015hlp.org/ wp-content/uploads/2013/02/Monrovia-Communique-1-February-2013.pdf
- Atun R, Jaffar S, Nishtar S, Knaul FM, Barreto ML, Nyirenda M, Banatvala N, Piot P.Improving responsiveness of health systems to non-communicable diseases. The Lancet2013, 381; 690-697
- UN Food and Agriculture Organization/World Bank. Food Systems and Poverty. Rome: FAO, 2001.ftp://ftp.fao.org/docrep/fao/004 /ac349e/ac349e00.pdf
- Arab Water Council. Perspectives on Water and Climate Change Adaptability. Vulnerability of Arid and Semi-Arid Regions to Climate Change http://www.worldwatercouncil.org/fileadmin/world_water_council/
documents_old/Library/Publications_and_reports/Climate_Change/PersPap_09._Arid_and_Semi-Arid_Regions.pdf - Kurlansky M. Salt. A World History. London: Penguin, 2003.
- Chen J, Wu X, Gu D. Hypertension and cardiovascular diseases intervention inthe capital steel and iron company and Beijing Fangshan community. Obesity Reviews. 2008, 9 Suppl 1:142-145.
Acknowledgement and request
Conflicting or competing interests: I am president of the International Association for the Study of Obesity, and founder of the International Obesity Task Force. I do not regard these as competing interests.
Readers may make use of the material in this column if acknowledgement is given to the Association. Please cite as: James WPT. Towards 2015-2025. [Column]. Website of the World Public Health Nutrition Association, February 2013. Obtainable at www.wphna.org.
All contributions to this website are the responsibility of their authors. They should not be taken to be the view or policy of the World Public Health Nutrition Association (the Association) or of any of its affiliated or associated bodies, unless this is explicitly stated.