2012 October blog
Geoffrey Cannon

São Paulo. Barbara Burlingame is the hero of this month. High time too. She is a senior official at the UN Food and Agriculture Organization, and a leading authority on the composition of food. This is vital work, not least because there are more foods in the world, especially in the tropics, than those included in the 'classic' food composition manuals published in temperate countries like the US and UK. More than this, Barbara is also one of the leaders within the UN system who advocate the food-based approach to nutrition and health, and who also believe that the best and most reliable way to alleviate food insecurity and nutrient deficiency is to give all possible support to small farmers, so that they can themselves sustain and nourish their families and communities.
More on Barbara at the end of this column. This month I begin by continuing to reflect on what we mean by 'cause', with obesity as the example, and continue my series on why I believe that living and working in the global South gives us a better understanding of nutrition and public health.
Obesity (and many other things)(2)
Causation, truth, and relevance
Access last month's column here

What causes obesity? Leptin, sloth (or trade agreements), takeaway pizzas, corn syrup, food addiction, or running deficiency? Or what else, and so what?
Here is the second of what have now become three reflections on causation. Those people in a position to prevent or control disease, or to protect and promote well-being, need to agree on what causes these conditions. They also need to have a good understanding of what 'cause' means, and what is meant by saying that X is the cause of Y or (not the same thing) that X causes Y. Otherwise they will be stuck.
Take obesity. The Political Declaration of the UN High Level Meeting on NCDs enjoins all actors including national governments and health professionals, to prevent and control non-communicable diseases, including obesity (1). This implies that there is some general agreement on what causes obesity, and therefore on what will prevent and control it. But there is no agreement, and therefore fat chance of prevention or control.
Elaborated from last month, some people say that the cause of obesity is a defect in carbohydrate metabolism, or else leptin resistance, or else as I now read, a 'hyperphagic phenotype' associated with the 'FTO' gene (2).Others say obesity is caused by excess of calories, or fatty sugary food products, or high-fructose corn syrup. There again, some say that obesity is caused by unwise personal choices, others say by yo-yo dieting regimes, and others say the cause is advertising and promotion of energy-dense hyper-palatable ultra-processed snacks and soft drinks.
But yet others say that the cause is price, or poverty, or induced catch-up growth, or in Mexico, the North American Food Trade Agreement (NAFTA). And there is more! Others say that the cause is greed, lack of will-power, food addiction, or failure to keeping on running. Meanwhile the boys from Coke™ seem to be putting across the notion that obesity is a physical activity deficiency disease. How come so many discordant voices? Isn't science supposed to come up with the answer, QED?
This is a tar-pit. No wonder so many consumers are confused and so many policy-makers are cynical. And obesity is just one example! Try a list of the proposed causes of diabetes, or heart disease, or come to that, well-being (3); or if in the mood to contemplate other big pictures, the world financial crash, or the invasions of Afghanistan.
You may now be feeling that discussion about 'cause' is intellectual fiddle-faddle, but sorry, it's basic. To repeat, the relevant actors, including national governments and international organisations, and indeed public health and nutrition professionals, can hope to prevent and control obesity and chronic non-communicable diseases, when and only when they agree on their cause, or (not the same thing) causes (4).
Truth, facts, relevance and ideology
To see what goes on, we need to understand what the term 'cause' means, and may be taken to mean. For a start, the account people give of what causes what, usually has little or practically nothing to do with what's 'true', in any final sense. What's meant is usually something less grand and more workaday, like 'consistent with the current relevant facts'. Nor is causation a fact. A claim of causation is an assertion, a judgement, an inference from evidence, which is to say sets of facts, or to be more precise, sets of facts of types that are understood, accepted or favoured (5).
We also need to be aware of where we are coming from. Anybody can see that accounts of causation are largely determined by temperament, training and knowledge, and general point of view – ideology, if you like. Hence Abraham Maslow's 'Law of the Instrument', often expressed as 'If you are holding a hammer, everything looks like a nail' (6).
That is to say, deciding what is the cause of what, is a matter of attitude and judgement. Of known sets of facts some people favour some, other people favour others. Last month I gave two examples. One contrasted the types of response a pathologist and a lawyer might give, in the same situation, to the question 'what caused this death?' Characteristic responses are shown in the text of the slides below:
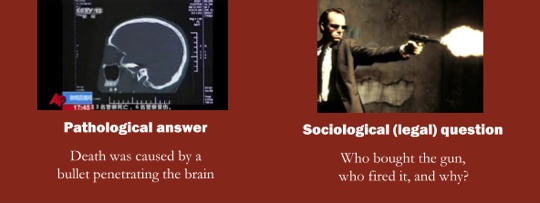
Asked what caused the same event, pathologists give 'how?' and 'what?' answers, while lawyers also address 'why?', 'who?' and 'when?' questions
Pathologists give their answers, and lawyers ask their questions, designed to guide a final formal judgement. Now back to obesity. The second example I gave last month contrasted how a biochemist and a sociologist characteristically might respond, asked to say what causes obesity. Again, see the text of the slides, below.
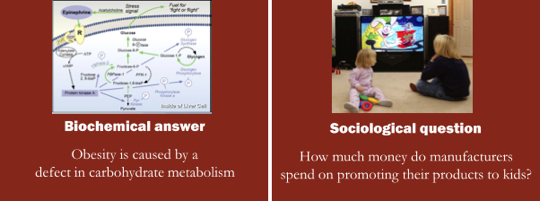
Biochemists, like pathologists, also give 'how?' and 'what?' answers, while sociologists, like lawyers, also address 'why?', 'who?' and 'when?' questions
'The contrasts have key points in common. The closed medical and biochemical answers address 'how?' and 'what?' questions. They are descriptive, detached and neutral, quantitative, and objective in the sense of being removed from time or place. They tend to state 'the cause of X is...' implying that there is a one and only cause. They are solid and focused.
The open legal and sociological questions do not ignore 'how?' and 'what?', but also raise further 'why?', 'who?', and 'when?' questions to which answers are needed. They are evaluative, engaged and tendentious (7), qualitative, and subjective in the sense of being rooted in time and place. They tend to say 'X is caused by...' which allows several or a cascade of causes or possible causes, among which choices and decisions about relative relevance and importance have to be made. They are malleable and diffuse. It is easy to see which of the two types of response is, in the usual sense now used of 'science', the more 'scientific'.
Nutritionists and causation
Sticking with the same example of obesity, I now come to our field of study and activity. What do nutritionists have to say about what causes obesity? And what do public health professionals say? This is an intriguing question, because here I am addressing readers concerned with public health nutrition.
Clinical nutritionists – the endos
Nutritionists, at least those who see themselves as 'scientists', have a range of interests and beliefs, but can be seen as split into two schools. Clinical nutrition, the type with greater prestige, is a precise discipline and profession, mainly concerned with animal and human laboratory experiments, the world inside bodies, and the biochemical and physiological mechanisms by which specific nutrients affect metabolism and other functions. To clinical nutritionists it is what goes on within the body that is most important. That's what they know. That is their 'truth', or in philosophical terms, their 'universe of discourse'.
The focus of clinical nutritionists is on endogenous, internal causes, so they can be called the 'endos'. This type of nutrition is usually practised by people with relatively tidy minds and with a low tolerance of confusion.
On what causes obesity, nutritionists whose predisposition has led them to be trained in this 'hard' approach, are therefore liable to give the same type of answer as biochemists, as illustrated above. Indeed, plenty of senior nutrition scientists are physicians or biochemists. The exact answer would depend to some extent on the special knowledge of the person giving the answer. Their discourse is much the same as that of pathologists: descriptive, detached, neutral, objective.
Applied nutritionists – the exos
The second school, which has less prestige, is sometimes called 'applied nutrition' (8). This has much in common with what is now the downgraded profession of community dietetics. It is a relatively diffuse discipline and profession, mainly concerned with group and population field interventions and the world outside the body, and with the impact of foods and diets as well as nutrients on diseases and patterns of disease. To applied nutritionists it is what goes on outside the body that is most important. That's what they know. That is their 'truth'.
The focus of applied nutritionists is on exogenous, external causes, so they can be called the 'exos'. This type of nutrition is usually practised by people with relatively adventurous minds, with a high tolerance for alternatives.
So on what causes obesity, nutritionists whose predisposition has led them to be trained in this 'soft' approach might give the same type of answer as epidemiologists. Indeed, plenty of senior applied nutrition scientists are epidemiologists. Again, the exact answer would depend on the expertise of the person giving the answer. This is a reason why panels of specialists are convened by relevant UN agencies, national governments and other authoritative bodies, to come up with general shared consensual agreements that can become the basis for recommendations, and then public policies and actions. Much depends on who is invited to join such panels, and where they are coming from.

Nutritionists who take a step beyond biochemistry see causes in the outside world. Public health professionals go far further out and engage in politics
One food-based view on causes of obesity (9) – there are plenty of others including some that are nutrient-based (10) – is illustrated above (left): 'Obesity is caused by energy-dense fatty or sugary fast food'. The discourse of this school of nutritionists goes some way towards that of sociologists, in that it is evaluative and engaged. It gives more scope for debate and disagreements. However, applied nutritionists who see themselves as 'scientists', as they usually do, are therefore likely to insist that their analyses and judgements are true, and that other views and conclusions are in error.
Public health nutritionists
So where do public health nutritionists fit, in this picture? The question is not simple. Unlike physiology, biochemistry, medicine, law, epidemiology, or clinical nutrition, public health nutrition does not have a generally shared set of principles that include guidance on causation, in general or in specific instances such as obesity (11). This may be a matter of time, or it may be inevitable. Most of the professionals whose work most powerfully impacts on public health nutrition, such as sanitary engineers or senior officials in the World Trade Organization, do not identify themselves as public health nutritionists.
When nutrition comes first
Of the rest, the first type are nutritionists with a commitment to public health, which I think makes them applied nutritionists who very sensibly have taken on a more resonant title. Their views on causation are therefore like that shown in the caption to the slide above (left). Specifically, on the causes of obesity, public health nutritionists of the first type have a range of views. The conservatives are more inclined to say that obesity is caused by excess consumption of nutrients such as fats and sugars, usually on the grounds that these are energy-dense or else supply energy and nothing else. The progressives are more inclined to emphasise categories of food and food products such as fast foods and sugared drinks. In this century the force has been with the progressives (12).
When public health comes first
Most of the rest are public health specialists who have special knowledge of or commitment to nutrition. Public health professionals (13), even if practically all their work is engaged with food and nutrition, are a very different breed from applied nutrition scientists. Indeed, while their work includes research, and while some are academics, nutritionists usually would not see them as scientists. Nor are they, in the biological or 'hard' sense. Inasmuch as they are seriously concerned with the condition of society, the more learned of them can be classed as social scientists. Their take on the causes of obesity is similar to that of lawyers and sociologists, as illustrated by the caption to the slide above (right).
Most public health professionals, even when involved in investigation, are more interested in action. Public health is less a science, more a movement. If the state of public health was generally seen as ideal, the profession might be more inclined to scholarship. But the systematic privatisation of public health, since the 1980s, an aspect of what remains the dominant global political and economic ideology (14), has meant that the leaders of the profession now tend to be activists. .
It's probably accurate to say that for most people engaged in public health, their work is an expression of a commitment to social justice (15), and that they see their scientific and technical knowledge, as civil engineers say, or city planners, or food policy experts, or international civil servants, or as physicians or epidemiologists – or nutritionists – as the means within their capacity, to greater liberty, equality and fraternity. Given this vista, the question of what causes obesity – or indeed any other public health crisis – becomes vast, because public health engages with social, ethical, cultural, political, economic, environmental and other domains (16).
It is no wonder that orderly scholars insist that the cause of obesity is a defect in carbohydrate metabolism! This is, after all, not wrong. But what is right? This is my topic for next month. As a hint, I propose that we first need to set aside notions of what is or may be 'true', and instead focus on what is relevant, and on what works. In public health, we should be less like clinicians and more like lawyers.
Until next month! And if you are participating in the SLAN conference in Havana, Cuba, I have just been told by the excellent people on the scientific committee that I will have a slot on Friday morning to develop the themes in this and next month's column.
References and notes
- After a lot of wrangling, the Political Declaration sort-of includes obesity as a non-communicable disease.
- Cecil J, Tavendale R, Watt P, Hetherington M, Palmer C. An obesity-associated FTO gene variant and increased energy intake in children. New England Journal of Medicine 2008, 359, 2558-2566. The phrase 'hyperphagic phenotype' comes from this paper. A gem!
- Now I read that dementia is a form of diabetes of which a cause is fast food (Trivedi B. Eat your way to dementia. New Scientist, 1 September 2012), while all along, I thought the cause was aluminium. (Cannon G. Water: Is it driving us mad? Telegraph Magazine, 20 September 1987). Drat!
- If 'general agreement' means that the transnational manufacturers of ultra-processed products must be part of the agreement, there never will be general agreement on the causes of obesity and diet-related diseases.
- Rothman K, Greenland S. Causation and causal inference. [Chapter 2]. In: Rothman K, Greenland S (eds). Modern Epidemiology. Second edition. Philadelphia PA: Lippincott, 1999.
- Maslow A. The Psychology of Science. A Reconnaissance. New York: Harper and Row, 1966.
- 'Tendentious' is used here in its original and proper neutral sense of 'having an underlying purpose' or 'tending towards a conclusion'.
- 'Applied nutrition' is a term not much used now. There was once a journal called Clinical Nutrition/Applied Nutrition, but I think it changed its name to something more auspicious. There are however plenty of nutrition professionals who are not clinicians, and I can't think of another term.
- Applied nutritionists, in common with public health professionals concerned with nutrition, now tend to focus not so much on nutrients (except in the case of deficiency diseases) as on foods, and on dietary patterns.
- For example, it remains generally agreed that excess consumption of fat, and saturated fats in particular, is the chief dietary cause of cardiovascular disease, but there is a growing minority view that the main cause is excess 'carbs', or else sugars.
- Yes, there is a very wide range of ideology within the profession of epidemiology, for example. But there is a shared set of general principles; whereas while clinical nutrition and applied/ public health nutrition apparently have a common topic, any statement offered as a unifying principle would be pretty abstract. And as the opening paragraph of this account of causation indicates, there is not much common ground between clinical nutritionists and public health professionals committed to nutrition.
- As witness World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases. Report of a joint WHO/FAO expert consultation. WHO technical report 916. Geneva: WHO. 2003. But this may change. Powerful policy-makers are insisting that the only evidence worth weighing comes from systematic literature reviews (SLRs) of randomised controlled trials (RCTs) and other statistically powerful, very expensive interventions. Since RCTs work for drugs and don't work for food, the results of such SLRs will always tend to show that food has little or nothing to do with obesity. So what is good evidence? This is the topic of another riff.
- There is no one word for a public health specialist. Is this significant?
- Garrett L. Betrayal of Trust. The Collapse of Global Public Health. New York: Hyperion, 2000.
- Socialism. For many, a loaded word. But then, so are 'capitalism' and 'imperialism', terms which champions of economic and political globalisation are now happy to use, and quite right too. While public health has technical aspects, all those who are professionally committed to greater social equity and the promotion of human rights are almost by definition socialists. They may discover this as a result of their professional commitment, or they may bring their existing ideology to bear on the protection and promotion of public health.
- World Federation of Public Health Associations. The Istanbul Declaration. Health: The First Human Right. May 2009. Obtainable at: www.wfpha.org. Pdf also available here.
Being in the tropics (2)
Life is all around
Access the November 2010 column here
Access the April 2011 column here
Access the January 2012 column here
Access last month's column here

Reasons to live in Brazil: couples of toucans in our garden, and geckos that emerge in my study at night and remind me to shut the lid of this computer
Here is the second in my new series of stories, begun last month. These consider why I as somebody engaged with public health, food and nourishment, a citizen of the global North, feel that only now do I now know what I am thinking, speaking and writing about, because of living and working in the global South. It will be good to know if what's here resonates with readers who have also made moves like mine.
My own stories are about aspects of Brazil, which is where I am. Needless to say, people in Brazil have a great variety of experiences of life. So it's maybe more accurate to say that what's here is aspects of being in the tropics. Some are dull, such as book covers going mouldy, storms outing the electricity, the occasional drug-crazed bandit crashing through the forest below our house, and give us this day our daily beans. But hey, we adjust.
All life is here
Last month I wrote about food. This month is about life. Read on please, and you will see the connection with food and nourishment. (For more on the topic of life, you are referred to items in four other columns: see the links above).
When European friends and colleagues first asked me what it was like being in Brazil, I said I was reminded of the motto of the now-defunct UK Sunday popular paper The News of the World: 'All human life is here'. Not only human either, as illustrated by the photographs above, both of which I took while sitting at my desk right here where I am now. One (left), is in early morning, and a couple of toucans in the trees above our garden. The other (right), is in late evening, and one of the family of geckos that come down from a shelf under the ceiling of my study, to catch moths and mosquitoes that unwisely settle inside the window in front of me with its view of our forest.
For anybody from a temperate country, who has seen toucans only in books or zoos or in films, it is glamorous hearing and seeing them real, live and free. I feel the same way when in our garden I watch tiny wild bees, iridescent humming-birds and big blue butterflies working, feeding and dancing. And inside, it is a new experience for me, sharing a home with other forms of life. Here we are not talking pot plants, which stay put, or domestic animals, that are dependent (1). They are wild, like the indoor little lizards that poo on my desk at night, and the hornets that construct their exquisite vespiaries inside as well as outside our house. The warmth of the climate, and the corresponding design of the house with its verandahs, dissolves the differences.
What all such simple experiences have done for and to me, is make me admit the most fundamental aspect of life beyond conventional science, which is life itself. Science is or should be a wonderful tool, but it is not reality. Our thoughts and dreams can be tracked with marvellous machines whose rays penetrate our brains, but what is shown on a screen is tracks of our dreams and thoughts, not our dreams or thoughts themselves. These have their own life, even if evanescent.
In the midst of life
Typically, people who live in the tropics, outside big cities, are aware of life as we all should be, in part because of the dark side. For them death is usual. Regular experience of death gives us a reliable sense of life. There's plenty here. On the three hour drive from Rio over the Petropolis mountains to the next state of Minas Gerais where I live, almost as often as not there is a overturned truck or smashed car, and over the years I have passed by a number of appalling multiple crashes. There is a lot of killing done here too, of cockroaches (ugh!), mosquitoes, the occasional snake; and from time to time hornets when they nest inside the house, though this makes me feel bad.
Where I live, normal death is not treated as obscene – behind the hospital curtains. After an aunt of my wife Raquel died last year, the whole family went to pay their respects to her displayed in an open coffin, her daughters wailing by her side, the men-folk talking business or politics in the corners of the room. This was impressive. When Kenai, one of our young half-Siamese cats, was killed by a car in May, it felt natural to me to take Korda his brother out to show him what had happened, and I watched, fascinated, as Korda seemed to be understanding by licking Kenai's body for a long time, and afterwards becoming more reserved, as he is now.
Good food goes bad
Now then, I come to life, food and nourishment. One of Michael Pollan's 'food rules' (1) is: 'Eat only foods that will eventually rot'. I prefer my snappier version, which is: 'Good food goes bad'. A variation is: 'Long shelf-life leads to short human life', which is not altogether accurate, because these days people with money for drugs and surgery can totter on for decades with stented or bypassed gummed-up arteries.
On the matter of life, food and nourishment, I am on the side of the hippies. It has always seemed absurd to me, to claim that a processed product whose chemical analysis is identical with that of a fresh food, is therefore its equivalent. The obvious objection to this silly idea is that the identity is only of the constituents being measured, by methods then available, with assumptions then current, which is a long way from being the same thing (2). Furthermore, it is perfectly possible that in say 50 years' time, the current 'official' micronutrients will be seen as unimportant, relative to many other bioactive compounds whose function is now poorly understood, or unknown.
But the more fundamental objection is that fresh food is alive, whereas chemically formulated products are sterile (3), dead (4). It is also perfectly possible that much of the benefit of fresh food is from the life-forms it contains that are off the nutrition science map – the many species of beneficial and commensal microbes.
At the Rio2012 conference this April I was confronted by a distinguished nutrition scientist. She told me that in common with US colleagues who the week before had attended the Federation of American Societies for Experimental Biology (FASEB) conference in San Diego, she had criticisms of the Association's publications. I asked her to be specific. 'Your column, for a start', she said. Ouch! But I see why. Thus in my columns I do say from time to time, of some point that seems pretty basic to me: 'you won't see this featured in a nutrition science textbook or learned journal'. Maybe I'm wrong, but I can't recall any chapter, section or reference in what are known as 'mainstream' textbooks or journals to live food as such, or to microbial species contained in live food other than those that are dangerous. If I am right, or more or less so, and if pointing this out gives offence, well sorry, but I think the books need a radical rewrite.
Reference and notes
- Pollan M. Food Rules. An Eater's Manual. London: Penguin, 2009.
- Assumptions. Chemically, trans-fats are mirror images of polyunsaturated fats, and so until fairly recently were assumed to be identical. Wrong!
- Have you ever wondered why manufacturers make such a song and dance about 'food safety'? The reason is obvious: sterile products are safe, in the sense that they don't contain bugs. Myself, I enjoy live food with its many millions of microbes per mouthful, and can't remember the last time I got acute guts-ache. Anyway, what's so terrible about the occasional transient bout of 'food poisoning', even when it doubles you up at the time? This way also we train our immune systems. Perhaps (half in jest) this suggests a new food rule for Michael Pollan's next edition. 'Make sure your food is stuffed with bugs'.
- Let's be a little more precise, here. In one usual sense, all food is dead. We don't eat animals when they are alive, as anacondas may devour a pig, and as my geckos snap up flies; and my lettuce for lunch today came plucked out of the ground. True. The life in fresh food is in the bugs that cause it to rot, and in its qualities that nourish them. This difference is measurable; but as said above, the only accounts I have seen in mainstream nutrition textbooks and journals concern pathogenic bacteria. This is helpful to the manufacturers of dead food products.
Barbara Burlingame
Meanings of food and nutrition
So much knowledge of early cultures is contained within traditional foods and their cultivation, and they have a direct impact on the physical, emotional, mental and spiritual health of indigenous communities. Indigenous …plant foods… provide important economic benefits, such as helping create self-sufficient communities and establishing a strong foundation of food security.
We believe the information can be a help to those in nutrition, agriculture, environmental and health education, and science, including policymakers. Nutritionists can use the information to try and correct imbalances in certain regions. For example, we discovered in research that the Pohnpei district community in the Federated States of Micronesia was severely deficient in vitamin A, despite the fact that a species of banana rich in vitamin A beta-carotenes was indigenous to the region. Once we determined the nutritional composition of the banana, we were able to educate the people about its benefit and encourage them to eat the local fruit, which helped reverse the deficiency.
Barbara Burlingame
Indigenous People's Food Systems, 2009
It's thrilling to read a senior nutrition scientist and food policy leader, speaking and writing about the mental, emotional and spiritual health of communities. As well as these being a prime concern of Barbara Burlingame personal, this approach is a sign of things to come and things that have already arrived, at the UN Food and Agriculture Organization. Exciting times!
Acknowledgement and request
Conflicting or competing interests: All the places I have worked have helped to shape my judgement and sometimes I wonder if these can amount to competing interests. Probably not. Reviewers of this column are Fabio Gomes and Claudio Schuftan. Readers may make use of the material in this column if acknowledgement is given to the Association, and WN is cited. Please cite as: Cannon G. Causation, truth and relevance, and other items. [Column]. Website of the World Public Health Nutrition Association, October 2012. Obtainable at www.wphna.org.
All contributions to this website are the responsibility of their authors. They should not be taken to be the view or policy of the World Public Health Nutrition Association (the Association) or of any of its affiliated or associated bodies, unless this is explicitly stated.